A reflection on humanitarian practice between conspiracy theories and sloppy controls.
For irresponsible that it may sound, facing prevention measures in Mali, I must confess that I actually find what I see around me somewhat reassuring: if these are the measures of containment and still the epidemic remains largely confined to Guinea, Liberia and Sierra Leone, then maybe one should reflect on the panicking about global contagion and on the old discipline-and-control story.
I have just come back from my fieldwork in Mali and Senegal. This is actually the frontier of the much talked-about Ebola epidemic: Mali shares a 800 km long boundary with Guinea, one of the countries most heavily hit by the virus (approximately 2,000 cases so far reported). I was based in Bamako, Mali’s capital, which lies only 120km from the border with Guinea, along a trafficked route connecting the port of Conakry, Guinea’s capital city, to landlocked Mali. Senegal shares a borderline with Guinea too. Individuals infected from Ebola virus were detected in both in Mali and Senegal, and in both cases they were reportedly coming from Guinea. The only person that was identified as a virus carrier in Senegal was immediately isolated and treated successfully: the country was officially declared – provisionally – Ebola-free on 17th October. These numbers, however, should be taken cautiously, given known problems with the capacity that several African governments have to collect, store and process data (see Morten Jerven’s Poor Number). In Mali, by contrast, six cases have been detected during the last few weeks, resulting in five fatalities: the first occurred the day before I arrived in Mali, the second and third ones the day after I left Bamako.
As any other traveler, then, I had the opportunity to experience the quality of the control, barriers and protection devices set up by the local governments, international organizations and NGOs to manage the crisis at the peak of the emergency, as well as to observe the reaction of the local society to the threat of a pandemic. In the following days I could complement my experience by exchanging views with several humanitarian workers engaged – in different capacities – in the management of the crisis. The impressions herein reported, so, are not meant to be an exhaustive and objective account of the responses implemented by Mali and the international community to the alleged advancement of the Ebola wave. Instead, and less ambitiously, this is nothing but the field notes of a (hopefully) reflexive observer that found itself more or less by chance at the storm centre: i.e., at its periphery, and ever advancing frontier.
Once in Bamako airport, while queuing in line and waiting for customs control, travelers are approached by doctors in white coat and half-mask. A young doctor pointed a sort of strange gun at people’s neck, from a distance: that is the tool supposed to measure fever. Concerning the Ebola crisis prevention, this is by far the most sophisticated and technologically advanced tool of public health I have seen and heard of in Mali. Nevertheless, the relevance of fever measurement is questionable: it is a well known fact that individuals can be vehicles of the virus during three weeks without manifesting any symptoms of the hemorrhagic fever. Secondly, despite the fact that children are often the privileged vehicles of the disease, they seldom receive attention (the first victim of Ebola in Mali was a young girl). Thirdly, and more disturbingly, when I was inspected, my body temperature, as measured by that odd tool, resulted to be a quite unrealistic 35 degrees Celsius. My neighbor was 34 degrees. And so on: unless believe in a sudden wave of collective hypothermia under the scorching African sun, we are probably allowed to raise some doubts about the reliability of the main tool deployed along the frontier of Ebola to prevent the spread of one of the most lethal viruses ever.
One should note that Bamako airport is border post is probably the best equipped in the whole country. Reportedly, there is only one single border post that performs some sort of rudimentary medical inspections along the immense boundary with Guinea. Aside from that, people keep on moving back and forth across the borders without restrictions, as they did for centuries: no inspections and supervisions from state authority. At the border post located by the Malian city of Kayes, a strategic hub on the way to Guinea, Mauritania and Senegal, doctors reportedly lack not only the functioning equipment and adequate infrastructure, but also white coats, gloves and half-masks that are crucially needed for self-protection. In some instances, the timely referral to Malian public clinics of individuals who allegedly contracted Ebola, a habit that international humanitarian agencies are struggling to support, resulted in the panicking and flight of medical personnel. According to a quite widespread rumor, all individuals who show up at clinics for medical consultation with symptoms that may lead one to suspect Ebola are indiscriminately quarantined prior to any further medical inspection that might prove or disprove the diagnosis. As a consequence, people simply affected by malaria or a cold are locked in, in close contact with those who may actually have Ebola, thus favoring the contagion.
Irrespective of the truthfulness of these claims, their mere existence in social discourses and perceptions is enough to discourage people from reporting suspicious cases to medical facilities, thus further facilitating the progression of the epidemics. In the meantime, the most diverse theories about the origins of Ebola are thriving, and get popular unchecked credit. Most of them are teleologically oriented, and they draw on a widespread culture of suspicion, conspiracy and victim complex. So, Ebola has been introduced in Africa by white men to decimate Africans, as they did with HIV; no, it’s a deliberate invention of the pharmaceutical corporations to raise their profits (without known existing treatment?); it is part of an American plot to further militarize Africa, following their failure to establish Africom headquarters in the continent: what would be the need, otherwise, to send troops to Liberia? How can a military intervention stop a virus invasion? The most imaginative theory I have heard was spelt out by a European executive working for a mining company in Guinea, provisionally recovered in Mali: how happens that the Ebola crisis is striking uniquely the three countries – i.e.: Liberia, Sierra Leone and Guinea – where the most important diamond mines worldwide are based? According to my interlocutor, this would seem to prove beyond any reasonable doubt the evil role played in this plot by diamond transnational corporations, and De Beers above all, aiming to produce a spectacular increase of the price of diamonds in world markets.
Despite their anecdotal nature, the proliferation of these conspirative theories shows that an element that is lacking to stop the progression of the Ebola crisis, in addition to medical facilities, adequate monitoring tools and proper training for medical personnel, is social capital and mutual trust among citizens, the international community and state authority. Many observers have pointed out that the outbreak of a (limited) Ebola crisis would actually benefit Mali’s President Ibrahim Boubacar Keita, in as much as it would contribute to re-focus the attention of the international community on Bamako. Keita’s credit, both vis-à-vis the international community and its own constituency, has been seriously shaken by recent financial scandals and alleged corruption in the purchasing of public goods. These led the IMF to block throughout the whole summer the loans that were previously granted to the state of Mali to fund the post civil war recovery. The materialization of Ebola would therefore provide to Keita the much needed opportunity to divert the international community attention, relaunch his own political standing, and renew sustained fund-raising efforts vis-à-vis international aid agencies.
Aiming to show its commitment and goodwill, Mali’s government has proved extremely receptive and ready to approve the measures recommended by the international community to halt the virus’ spread. Leaving aside the consistent failure of Mali – as reported above – to adequately implement those measures and international standards, that can be attributed to many different causes including inadequate means, corruption, state weakness, etc., this political commitment has been translated into an impressive normative proliferation that deserves some attention. The Prime Minister has revealed that, under the pressure of unspecified international actors, his government had adopted 33 new legislative measures designed to tackle the progression of the virus, on 25th October only, that is to say a couple of days after the first case of Ebola was confirmed in Mali. Due to the perceptions of an uncontrollable emergency, and to the need for international support, new laws, normative standards and administrative measures are adopted by Malian authorities hastily, without careful scrutiny and widespread democratic consultations.
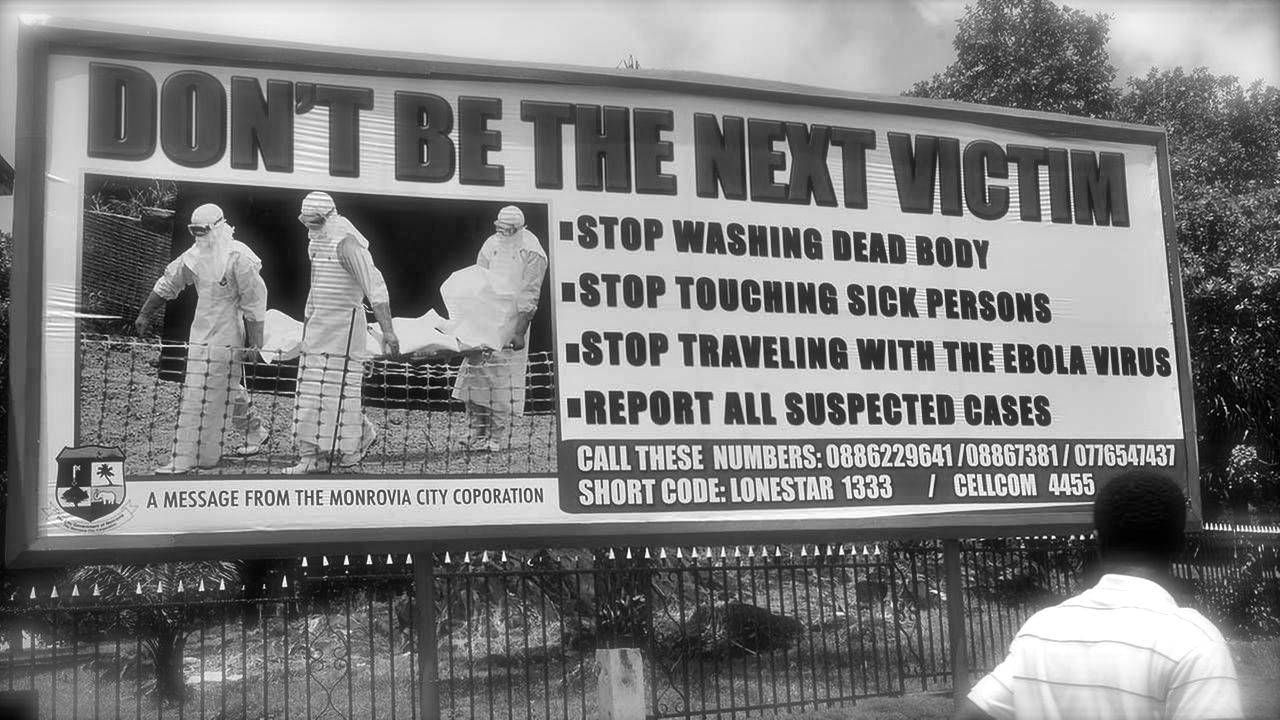
The normative production goes well beyond the legislative and administrative domains, and is aimed to regulate Malians’ daily lives. Advertisements on giant billboards along the main roads and during TV shows at all times on all chains are incessantly reminding to Malians how they are expected to behave in their daily lives and social relationships in order to contribute to the international crusade against Ebola. The regulation of daily lives thus fostered is meticulous and widespread: don’t embrace nor hug; don’t eat nor touch wild animals; wash your hands after every human contact. Such an articulated disciplining of everyday behaviors is not without reminding the paradigm of biopolitics described by Foucault. Prescriptions of good conduct intrude even in the most intimate and sacred spheres of private life, as mourning, funerals and ceremonies surrounding deaths are indeed among the most favorable opportunities to promote infection and the spread of the disease.
These considerations do not imply that public health imperatives don’t deserve attention. Nevertheless, from a moral point of view, these cannot be considered the only obligations at stake here. Instead, they interact with a wide set of moral values, with whom they may happen to compete. The priority attributed without further reflection to the imperatives of public health, irrespective of individual rights and competing duties, echoes the longstanding utilitarian tradition that aims to promote “the greatest good for the greatest number”. Interestingly, such a fortunate formula had been introduced by Jeremy Bentham, the same prolific author who put forward the idea of the Panopticon, that Foucault identifies as the supreme paradigm of the modern power to discipline and control. Discipline and control are today the fundamental strategies put forward by State actors, humanitarian agencies and international donors to brake and halt the spread of the Ebola epidemic: the former is pursued via normative production, both at legislative and behavioral level; the latter takes place at the state borders, at the “periphery of the evil”. Incidentally, they might both contribute to state-building practices, especially in the case of a state as weak and dysfunctional as Mali.
The fact that these measures are, on the ground, much less almighty and effective than expected by their promoters doesn’t deprive the argument of its significance. On the contrary, it might actually support it. On a personal level, I must confess that I actually find this ineffectiveness reassuring, somewhat paradoxically: if measures of containment are clearly not working, but still the epidemic remains largely confined to three states (Guinea, Liberia, Sierra Leone), then maybe the widespread panic of a global contagion is largely misplaced. The alarm about Ebola systematically raised by humanitarian agencies in the last few months was understandably aimed at attracting media coverage, mobilizing support and commitment from the international community and donors, and at raising the awareness of the general audience, both in the target countries and abroad. This approach has certainly provided a tremendous contribution to slow down the progression of the epidemic. Unfortunately, however, it has also contributed to foster an imaginary geography that depicts Africa in general as a place of danger, disease and promiscuity, along the lines of the worst orientalist tradition. This has further exacerbated a growing racist discourse in Europe.
It is worth remembering, however, that the humanitarian community is increasingly aware of the problematic side effects of its action. Interesting examples of reflexive approaches adopted by humanitarian actors vis-à-vis their own practices can be seen, for instance, here and here. Max Weber argued that utilitarianism is the only rational moral conduct, and it is therefore superior to any traditional or deontological approach. One century after Weber, however, some field experience allows to see how dangerous it can be to simply disregard and dismiss alternative normative approaches. Not only in the problematic field of public health, but also as a way of consistently questioning how healthy practices of state discipline and control are in actual terms.